







Risk factors for coronary artery disease (CAD) were not formally established until the initial findings of the Framingham Heart Study in the early 1960s.
The understanding of such factors is critical to the prevention of cardiovascular morbidities and mortality. See the image below.
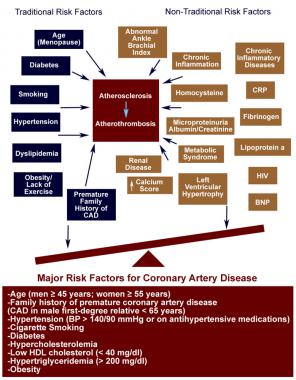
Traditional versus nontraditional risk factors for coronary artery disease (CAD). The expanding list of nontraditional biomarkers is outweighed by the standard risk factors for predicting future cardiovascular events and adds only moderately to standard risk factors. BNP = B-type natriuretic peptide; BP = blood pressure; CRP = C-reactive protein; HDL = high-density lipoprotein cholesterol; HIV = human immunodeficiency virus infection.
Risk factors for coronary artery disease
Conventional risk factors
- Older age: Over age 45 years in men and over age 55 years in women
- Family history of early heart disease
- Race: Among persons with CAD, the cardiovascular death rate for African Americans is reported to be particularly high; in Asians, low levels of high-density lipoprotein cholesterol (HDL-C), which are considered to be a risk factor for coronary heart disease, appear to be especially prevalent; South Asians appear to have a higher independent risk for cardiovascular disease as well.
Modifiable risk factors
- High blood cholesterol levels (specifically, low-density lipoprotein cholesterol [LDL-C])
- High blood pressure
- Cigarette smoking: Cessation of cigarette smoking constitutes the single most important preventive measure for CAD
- Diabetes mellitus
- Obesity
- Lack of physical activity
- Metabolic syndrome
- Mental stress and depression
Nontraditional or novel risk factors
High levels of the following are considered to be risk factors for CAD:
- C-reactive protein (CRP): High levels are related to the presence of inflammation and, according to some research results, may be associated with an increased risk of CAD development and heart attack
- Lipoprotein(a)
- Homocysteine: In the general population, mild to moderate elevations are due to insufficient dietary intake of folic acid, but homocysteine levels may also identify people at increased risk for heart disease
- Small, dense LDL-C particles
- Fibrinogen
Various medical conditions that can contribute to CAD include the following:
- End-stage renal disease (ESRD)
- Chronic inflammatory diseases affecting connective tissues (eg, lupus, rheumatoid arthritis)
- Human immunodeficiency virus (HIV) infection (acquired immunodeficiency syndrome [AIDS], highly active antiretroviral therapy [HAART])
- Xanthelasmata (raised yellow patches around the eyelids)
The following are also considered to be risk factors:
- Tissue plasminogen activator (tPA): An imbalance of the clot dissolving enzymes (eg, tPA) and their respective inhibitors (plasminogen activator inhibitor-1 [PAI-1]) may predispose individuals to myocardial infarctions
- Low serum testosterone levels: Have a significant negative impact on patients with CAD
- Hysterectomy: A study suggests that this becomes a risk factor later in life in women who have the surgery at or before age 50 years
- Lack of sleep
Identifying coronary artery disease
Direct plaque imaging
- Electron-beam computed tomography (EBCT) scanning: To identify coronary calcification; can reveal at-risk individuals and perhaps allow for medical monitoring
- 64-slice CT angiography: Bulky plaques may be identified in asymptomatic patients; the risk-benefit of using CT angiography in an asymptomatic patient for the identification of atherosclerotic plaques is still a subject of much debate
- Carotid intima-media thickness (IMT), pulse wave velocity (PWV), and the ankle-brachial index (ABI): Widely used, noninvasive modalities for evaluating atherosclerosis
Biomarkers
In a 10-year comparison of 10 biomarkers for predicting death and major cardiovascular events in approximately 3000 individuals, the most informative biomarkers for predicting death were as follows:
- B-type natriuretic peptide (BNP)
- CRP
- Homocysteine
- Renin
- Urinary albumin-to-creatinine ratio
The most informative biomarkers for predicting major cardiovascular events were BNP and the urinary albumin-to-creatinine ratio.
Source emedicine.com
Duc Tin Surgical Clinic
Tin tức liên quan

Performance diagnostique de l’interféron gamma dans l’identification de l’origine tuberculeuse des pleurésies exsudatives

A Mixed Phenotype of Airway Wall Thickening and Emphysema Is Associated with Dyspnea and Hospitalization for Chronic Obstructive Pulmonary Disease.

Radiological Approach to Asthma and COPD-The Role of Computed Tomography.

Significant annual cost savings found with UrgoStart in UK and Germany

Thrombolex announces 510(k) clearance of Bashir catheter systems for thromboembolic disorders
Phone: (028) 3981 2678
Mobile: 0903 839 878 - 0909 384 389