







Atherosclerotic cardiovascular disease (ASCVD)ddefined as acute coronary syndromes (ACSs), a history of myocardial infarction (MI), stable or unstable angina, coronary or other arterial revascularization, stroke, transient ischemic attack, or peripheral arterial disease presumed to be of atherosclerotic origindis the leading cause of morbidity and mortality for individuals with diabetes and is the largest contributor to the direct and indirect costs of diabetes.
The common conditions coexisting with type 2 diabetes (e.g., hypertension and dyslipidemia) are clear risk factors for ASCVD, and diabetes itself confers independent risk. Numerous studies have shown the efficacy of controlling individual cardiovascular risk factors in preventing or slowing ASCVD in people with diabetes. Large benefits are seen when multiple risk factors are addressed simultaneously. There is evidence that measures of 10-year coronary heart disease (CHD) risk among U.S. adults with diabetes have improved significantly over the past decade (1) and that ASCVD morbidity and mortality have decreased (2–4).
In all patients with diabetes, cardiovascular risk factors should be systematically assessed at least annually. These risk factors include hypertension, dyslipidemia, smoking, a family history of premature coronary disease, and the presence of albuminuria. Abnormal risk factors should be treated as described in these guidelines.
HYPERTENSION/BLOOD PRESSURE CONTROL
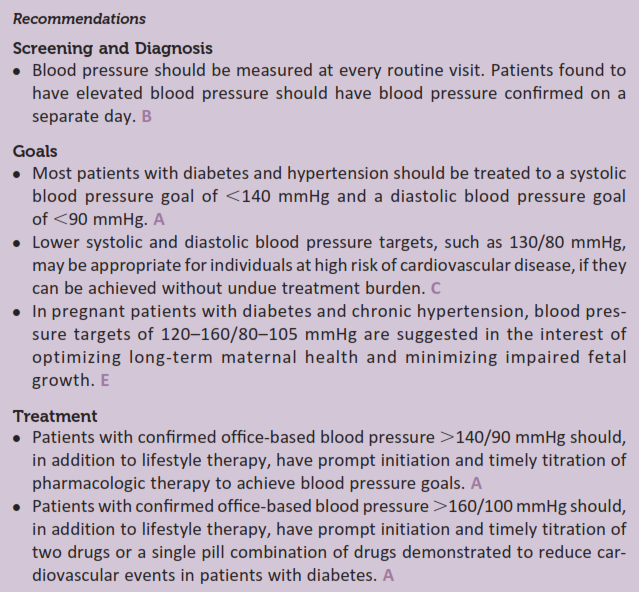
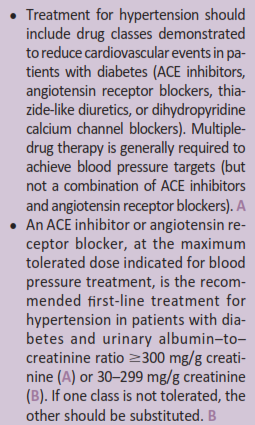
Hypertension, defined as a sustained blood pressure $140/90 mmHg, is a common comorbidity of type 1 and type 2 diabetes. The prevalence of hypertension depends on type of diabetes, age, sex, BMI, and race/ethnicity. Hypertension is a major risk factor for both ASCVD and microvascular complications. In type 1 diabetes, hypertension is often the result of underlying diabetic kidney disease, while in type 2 diabetes, it usually coexists with other cardiometabolic risk factors. Please refer to the American Diabetes Association (ADA) position statement “Diabetes and Hypertension” for a detailed review (5).
Source ADA 2017
Duc Tin Surgical Clinic
Tin tức liên quan

Performance diagnostique de l’interféron gamma dans l’identification de l’origine tuberculeuse des pleurésies exsudatives

A Mixed Phenotype of Airway Wall Thickening and Emphysema Is Associated with Dyspnea and Hospitalization for Chronic Obstructive Pulmonary Disease.

Radiological Approach to Asthma and COPD-The Role of Computed Tomography.

Significant annual cost savings found with UrgoStart in UK and Germany

Thrombolex announces 510(k) clearance of Bashir catheter systems for thromboembolic disorders
Phone: (028) 3981 2678
Mobile: 0903 839 878 - 0909 384 389