







In line with our commitment to provide world-class facilities and deliver excellence in clinical care, San Radiology recently installed the cardiac-capable Siemens FORCE CT Scanner (384-slice, Dual Source). In March 2015, in a world-first, San Radiology achieved the lowest dose of radiation ever reported for Cardiac CT imaging, according to the supplier Siemens Healthcare. Our average dose for Cardiac CT is significantly lower than the safety reference guidelines used for CT in Australia (in many instances up to 98% lower).
This Siemens FORCE CT produces extremely high quality and resolution images of the heart and its blood supply in less than 5 seconds.
Our experienced and subspecialised Radiologists (with Level II Accreditation by the Conjoint Committee for the Recognition of Training in CT Coronary Angiography) and CT Radiographers have been pioneers and industry leaders in the field of Cardiac CT in Australia. San Radiology has performed approximately 10,000 Cardiac CT examinations since the commencement of our Cardiac CT service in 2006, the year in which San Radiology was the first in Australia to install a dual-source CT scanner.
What is a Cardiac CT?
Cardiac CT (Computed Tomograph) is a collective term that includes:
- Coronary Artery Calcium Scoring (CACS)
- CT coronary angiography (CTCA)
- Functional Cardiac CT
.png)
.png)
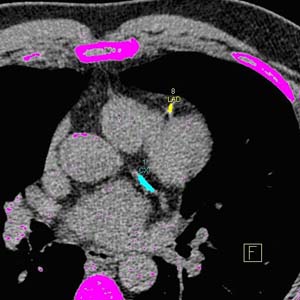
Cardiac CT is a painless procedure, which involves an enclosed X-ray tube spinning around the patient’s body generating hundreds of images (slices) of the heart in a single breath hold. In the case of a dual source CT, there are two X-ray tubes generating these images.
Coronary Artery Calcium Scoring (CACS)
This form of cardiac CT does not involve an injection of X-ray dye (see below) and assesses the amount of calcified atheroma (hardening of the arteries) to obtain a value (Agaston Score), which will give an indication of the risk of that patient having a significant cardiovascular event within the next 10 years. Similar to a raised cholesterol level, it tells us that the risk of heart disease is elevated when the Score is markedly elevated.
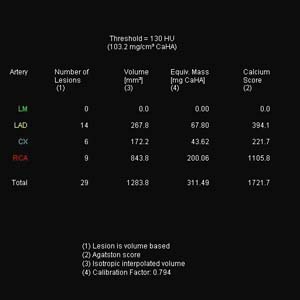
Coronary Artery Calcium Score showing calcium deposits on the coronary arteries
A value of 0 is an excellent predictor of having a very low risk. Other values are usually interpreted in combination with patient age and sex. The presence of calcium on an artery does not necessarily mean that the artery is severely narrowed. In order to obtain information about the severity of a potential narrowing of a coronary artery and to identify non-calcified fatty deposits, however, one may perform a CTCA.
CT Coronary Angiography (CTCA)
CT coronary angiography involves the assessment of the inside of coronary arteries using the Cardiac CT technique following the injection of X-ray dye (see below).
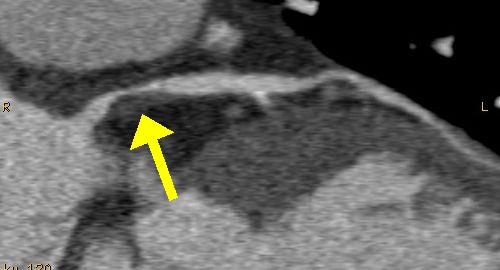
The X-ray dye (Iodine containing contrast medium, ICCM) outlines the coronary arteries permitting the assessment of significant narrowing of the arteries and abnormal atheroma deposits in their walls.
Functional Cardiac CT
This refers to obtaining additional information about the heart and its structures during the acquisition of a cardiac CT, such as the heart valves, wall thickness of the heart chambers and how well they contract.
Whether this information is available will depend on how the cardiac CT is performed. Techniques are now available to maximally reduce X-ray exposure to the patient. However, this may often lead to the functional data not being available. This type of information can be easily obtained with other tests such as cardiac echo without additional X-ray exposure.
Chest Pain Protocol
At the expense of a slight increase in X-ray exposure, it is possible to completely assess other structures in the patient’s chest, outside the region that contains the heart. This enables us to assess the thoracic aorta (blood vessel connecting the heart to the rest of the body), the pulmonary vessels (blood vessels connecting the heart to the lungs), lymph nodes and other mediastinal structures, the lungs and spine. Thus we may identify not only heart related causes of chest pain but pathology arising in other organ causing the symptoms.
Source www.sah.org.au
DucTin Clinic
Tin tức liên quan

Performance diagnostique de l’interféron gamma dans l’identification de l’origine tuberculeuse des pleurésies exsudatives

A Mixed Phenotype of Airway Wall Thickening and Emphysema Is Associated with Dyspnea and Hospitalization for Chronic Obstructive Pulmonary Disease.

Radiological Approach to Asthma and COPD-The Role of Computed Tomography.

Significant annual cost savings found with UrgoStart in UK and Germany

Thrombolex announces 510(k) clearance of Bashir catheter systems for thromboembolic disorders
Phone: (028) 3981 2678
Mobile: 0903 839 878 - 0909 384 389