







Who should have a Cardiac CT?
Before considering undergoing a cardiac CT, the most important step for the patient is to consult with their physician. This is because some cardiac CT uses are more appropriate than others, and the scan carries some risks from X-ray exposure and contrast dye administration.
As a result of our extensive experience of more than 4000 examinations, through careful patient selection and radiation reduction efforts, we have been able to minimise the risk to patients. There is close cooperation between our cardiac CT trained radiologists and many of the cardiologists associated with the Sydney Adventist Hospital (SAH) as well as numerous external referrers. Many of the abnormal findings have been correlated with conventional coronary angiography subsequently performed at the SAH.
Based on local experience and the result of international research, it is increasing accepted that the use of cardiac CT can be supported in the following settings:
- Patients with intermediate to high-risk profiles for coronary artery disease (eg. 2 or more of the following risk factors: Older than 45 years, high cholesterol, smoker, diabetes or family history of heart disease), but without typical symptoms (see below).
- Unusual (atypical) symptoms for coronary artery disease (such as chest pain unrelated to physical exertion), but low to intermediate risk profiles for coronary artery disease.
- Unclear or inconclusive stress-test (treadmill test) results.
In addition, in certain settings cardiac CT may provide additional information that could otherwise only be obtained through invasive angiography, or to clarify findings from other tests such cardiac echography or nuclear medicine studies. These indications include:
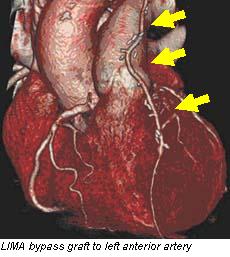
- Following previous cardiac surgery:
- Bypass graft assessment (to assess whether the grafts are still working)
- Investigation of complications of surgery
- Following coronary artery stent insertion (see notes below)
- Further assessment of tumours of the heart or its lining
- Assessment of the coronary arteries in patients in whom conventional angiography may very risky, eg. severe aortic valve disease..


Who should not have a Cardiac CT?
- Patients who have typical symptoms for significant coronary artery disease (especially typical chest pain, shortness of breath, or fatigue during heavy physical activity)
- Patients who have classic findings of significant coronary artery disease such as ECG or blood test findings consistent with a heart attack or angina
- Patients with contraindications to x-ray dye administration (see Risks of Cardiac CT for further information)
- Patients in whom the study is unlikely to be fully diagnostic, such as those with small coronary artery stents (less than 3mm diameter) or known severe coronary artery calcification
- Patients with known significant coronary artery disease and recurrence/worsening of symptoms
- Pregnant patients.
In many of these patients, first line assessment with conventional invasive coronary angiography is usually required following assessment by a cardiologist.
Source www.sah.org.au
Duc Tin Clinic
Tin tức liên quan

Performance diagnostique de l’interféron gamma dans l’identification de l’origine tuberculeuse des pleurésies exsudatives

A Mixed Phenotype of Airway Wall Thickening and Emphysema Is Associated with Dyspnea and Hospitalization for Chronic Obstructive Pulmonary Disease.

Radiological Approach to Asthma and COPD-The Role of Computed Tomography.

Significant annual cost savings found with UrgoStart in UK and Germany

Thrombolex announces 510(k) clearance of Bashir catheter systems for thromboembolic disorders
Phone: (028) 3981 2678
Mobile: 0903 839 878 - 0909 384 389