







Acute pericarditis is an inflammation of the pericardium characterized by chest pain, pericardial friction rub, and serial ECG changes.
The first and last stages of ECG changes are seen in the images below.
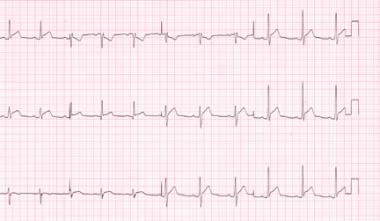
Stage 1 electrocardiograph changes in a patient with acute pericarditis.

Stage 4 electrocardiograph changes in the same patient as in the previous image, taken approximately 3 months after acute pericardial illness. The patient remained symptom free despite continued T-wave inversion.
Signs and symptoms
Chest pain is the cardinal symptom of pericarditis, usually precordial or retrosternal with referral to the trapezius ridge, neck, left shoulder, or arm. Common associated signs and symptoms include low-grade intermittent fever, dyspnea/tachypnea (a frequent complaint and may be severe, with myocarditis, pericarditis, and cardiac tamponade), cough, and dysphagia. In tuberculous pericarditis, fever, night sweats, and weight loss are commonly noted (80%).
Specific causes of pericarditis include the following:
Idiopathic causes
Infectious conditions, such as viral, bacterial, and tuberculous infections
Inflammatory disorders, such as RA, SLE, scleroderma, and rheumatic fever
Metabolic disorders, such as renal failure, hypothyroidism, and hypercholesterolemia
Cardiovascular disorders, such as acute MI, Dressler syndrome, and aortic dissection
Miscellaneous causes, such as iatrogenic, neoplasms, drugs, irradiation, cardiovascular procedures, and trauma
Diagnosis
Initial evaluation includes a clinical history and physical examination, ECG, echocardiography, chest radiography, and lab studies.
ECG can be diagnostic in acute pericarditis and typically shows ST elevation in all leads. The ratio of the amplitude of ST segment to the amplitude of the T wave in leads I, V4, V5, and V6 on electrocardiogram can be used to differentiate acute pericarditis (AP) from early repolarization (ER) and early repolarization of left ventricular hypertrophy (ERLVH), according to a recent study. When ST elevation was present in lead I, the ST/T ratio had the best predictive value for discriminating between AP, ER and ERLVH. The study involved 25 patients with AP, 27 with ER, and 28 with ERLVH.
Echocardiography is particularly helpful if pericardial effusion is suspected on clinical or radiographic grounds, the illness lasts longer than 1 week, or myocarditis or purulent pericarditis is suspected.
A chest radiograph is only helpful for diagnosis in patients with effusions >250mL. Patients with small effusions (less than a few hundred milliliters) may present with a normal cardiac silhouette.
Lab tests may include CBC; serum electrolyte, blood urea nitrogen (BUN), and creatinine levels; erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels; and cardiac biomarker measurements, lactate dehydrogenase (LDH), and serum glutamic-oxaloacetic transaminase (SGOT; AST) levels.
Management
Treatment for specific causes of pericarditis is directed according to the underlying cause. For patients with idiopathic or viral pericarditis, therapy is directed at symptom relief.
Pharmacologic treatment
Nonsteroidal anti-inflammatory drugs (NSAIDs) are the mainstay of therapy. These agents have a similar efficacy, with relief of chest pain in about 85-90% of patients within days of treatment. A full-dose NSAID should be used, and treatment should last 7-14 days.
Colchicine, alone or in combination with an NSAID, can be considered for patients with recurrent or continued symptoms beyond 14 days.
Corticosteroids should not be used for initial treatment of pericarditis unless it is indicated for the underlying disease, the patient’s condition has no response to NSAIDs or colchicine, or both agents are contraindicated.
Surgical treatment
Surgical procedures for pericarditis include pericardiectomy, pericardiocentesis, pericardial window placement, and pericardiotomy.
Pericardiectomy is the most effective surgical procedure for managing large effusions, because it has the lowest associated risk of recurrent effusions. This procedure is used for constrictive pericarditis, effusive pericarditis, or recurrent pericarditis with multiple attacks, steroid dependence, and/or intolerance to other medical management.
Patients with effusions larger than 250 mL, effusions in which size increases despite intensive dialysis for 10-14 days, or effusions with evidence of tamponade are candidates for pericardiocentesis.
Pericardial window placement is used for effusive pericarditis therapy. In critically ill patients, a balloon catheter may be used to create a pericardial window, in which only 9 cm2 or less of pericardium is resected.
Consider subxiphoid pericardiotomy for large effusions that do not resolve. This procedure may be performed under local anesthesia and has a lower risk of complications than pericardiectomy.
Source emedicine.com
PK Đức Tín
Tin tức liên quan

Performance diagnostique de l’interféron gamma dans l’identification de l’origine tuberculeuse des pleurésies exsudatives

A Mixed Phenotype of Airway Wall Thickening and Emphysema Is Associated with Dyspnea and Hospitalization for Chronic Obstructive Pulmonary Disease.

Radiological Approach to Asthma and COPD-The Role of Computed Tomography.

Significant annual cost savings found with UrgoStart in UK and Germany

Thrombolex announces 510(k) clearance of Bashir catheter systems for thromboembolic disorders
Phone: (028) 3981 2678
Mobile: 0903 839 878 - 0909 384 389