







Varicose Vein Surgery
Background
The description of varicose veins as a clinical entity can be traced back as early as the fifth century BCE.
Hippocrates, Galen, and others described the disease and treatment modalities, which are still used today. Throughout the centuries, surgical treatments have evolved from large open procedures to minimally invasive approaches.
Varicose veins represent a significant clinical problem and are not just a “cosmetic” issue because of their unsightly nature. The problem arises from the fact that varicose veins actually represent underlying chronic venous insufficiency with ensuing venous hypertension. This venous hypertension leads to a broad spectrum of clinical manifestations, ranging from symptoms to cutaneous findings like varicose veins, reticular veins, telangiectasias, swelling, skin discoloration, and ulcerations.
Varicose veins and even chronic venous insufficiency can be managed conservatively with stockings and compression. More aggressive management can be pursued for cosmesis, worsening cutaneous findings or symptoms despite conservative management, or if the patients prefer surgical management. Most procedures to treat varicose veins can be elective, and emergency treatment and workup is usually reserved for bleeding varicosities or if deep venous thrombosis(DVT) is suspected.
Anatomy
Two venous systems are found in the lower extremity, the deep and superficial (see the image below). The deep system ultimately leads backs to the inferior vena cava, then to the heart. The superficial system is found above the deep fascia of the lower extremity, within the subcutaneous tissue. Many superficial veins exist, but they all drain into the two largest: the great saphenous vein (GSV; also referred to as the greater saphenous vein) and the small saphenous vein (SSV; also referred to as the short, smaller, or lesser saphenous vein).
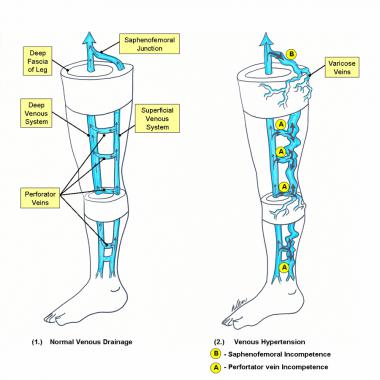
Schematic diagram of the deep and superficial venous systems of the lower extremity: (1) Normal venous drainage; arrows depict the flow of venous blood. (2) Venous hypertension bold arrows are pathways of venous reflux.
The GSV originates on the medial foot as part of the venous arch and receives tributaries from deep veins of the foot as it courses upward along the anterior aspect of the medial malleolus. From the ankle, the GSV continues along the anteromedial aspect of the calf to the knee and into the thigh, where it is found more medially.
From the upper calf to the groin, the GSV is usually contained within an envelope of thin fascia. Visualization of this fascial envelope is an important way of identifying the GSV with duplex ultrasonography. This fascial envelope often prevents the GSV from becoming significantly dilated, even when large volumes of reflux pass along its entire length. A normal GSV is typically 3-4 mm in diameter in the midthigh.
Along its course, a variable number of named perforating veins transverse the deep fascia of the lower extremity and connect the GSV to the deep system at the femoral, posterior tibial, gastrocnemius, and soleal veins (see the image below). The Cockett perforators, between the ankle and the knee, are a special group of perforating veins. Rather than directly connecting the superficial to deep venous systems, they connect the subfascial deep system with the posterior arch vein, which then empties into the GSV.
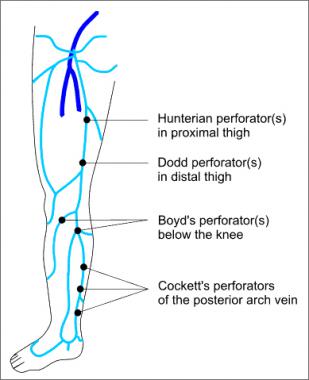
Named perforators along the greater saphenous distribution.
Besides perforating veins, the GSV has numerous superficial tributaries as it passes through the thigh (see the image below). The most important of these are the posteromedial and anterolateral thigh veins, found at the level of the midthigh, and the anterior and posterior accessory saphenous veins at the level of the canal of Hunter in the upper thigh, where a perforating vein often connects the GSV to the femoral vein.
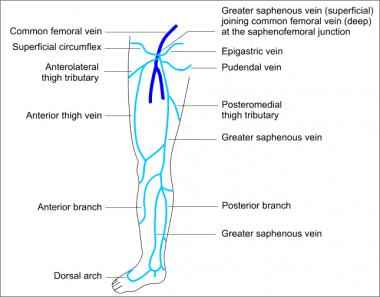
Major tributaries of the greater saphenous system.
Just below its junction with the common femoral vein, the GSV receives several additional important tributary veins. These include the lateral and medial femoral cutaneous branches, the external circumflex iliac vein, the superficial epigastric vein, and the internal pudendal vein. These tributaries are frequently involved in the reflux that leads to the appearance of surface varicose veins on the lower thigh or upper calf.
The termination point of the GSV into the common femoral vein, located proximally at the groin, is called the saphenofemoral junction (SFJ) in the English literature but is known as the crosse (ie, shepherd's crook) in the French medical literature (see the image below). The terminal valve of the GSV is located within the junction itself. In most cases, at least one additional subterminal valve is present within the first few centimeters of the GSV. Most patients have a single subterminal valve that can be readily identified approximately 1 cm distal to the junctional valve.
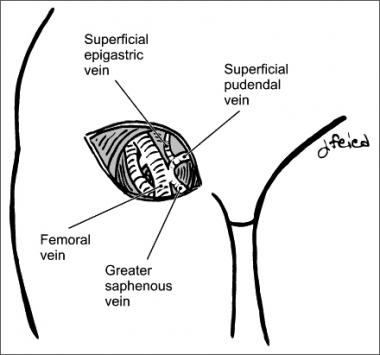
Saphenofemoral junction.
The saphenopopliteal junction (SPJ) is located behind the knee where the SSV joins with the popliteal vein.
Theo emedicine.com
Duc Tin Surgical Clinic
Tin tức liên quan

Performance diagnostique de l’interféron gamma dans l’identification de l’origine tuberculeuse des pleurésies exsudatives

A Mixed Phenotype of Airway Wall Thickening and Emphysema Is Associated with Dyspnea and Hospitalization for Chronic Obstructive Pulmonary Disease.

Radiological Approach to Asthma and COPD-The Role of Computed Tomography.

Significant annual cost savings found with UrgoStart in UK and Germany

Thrombolex announces 510(k) clearance of Bashir catheter systems for thromboembolic disorders
Phone: (028) 3981 2678
Mobile: 0903 839 878 - 0909 384 389