







Varicose veins are simply dilated, tortuous veins of the subcutaneous/superficial venous system. However, the pathophysiology behind their formation is complicated and involves the concept of ambulatory venous hypertension.
To understand this process, it is necessary to be familair with the anatomy of the lower-extremity venous system, as outlined above
In healthy veins, the flow of venous blood is through the superficial system into the deep system and up the leg and toward the heart (see the image below). One-way venous valves are found in both systems and the perforating veins. Incompetence in any of these valves can lead to a disruption in the unidirectional flow of blood toward the heart and result in ambulatory venous hypertension.
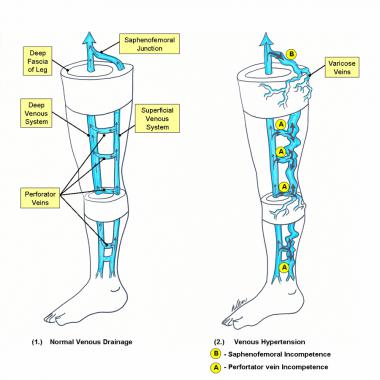
Schematic diagram of the deep and superficial venous systems of the lower extremity: (1) Normal venous drainage; arrows depict the flow of venous blood. (2) Venous hypertension bold arrows are pathways of venous reflux.
Furthermore, incompetence in one system can often lead to incompetence in another. In a study by Shami et al, the limbs of 59 patients with venous ulceration were assessed by color duplex ultrasound scanning. In 53% of patients only superficial venous reflux was found, in 15% isolated deep venous reflux was found, and in 32% a combination of deep and superficial venous reflux was found.
Incompetence in the superficial venous system alone usually results from failure at valves located at the SFJ and SPJ. The gravitational weight of the column of blood along the length of the vein creates hydrostatic pressure, which is worse at the more distal aspect of the length of vein (see circle A in the image above
Reflux at or near the SFJ does not always come through the terminal valve of the GSV, nor does it always involve the entire trunk of the GSV. Reflux can enter the GSV below the subterminal valve or even immediately below the junction, passing through a failed subterminal valve to mimic true SFJ incompetence. Reflux can also pass directly into any of the other veins that join the GSV at that level, or it may pass a few centimeters along the GSV and then abandon the GSV for another branch vessel, as depicted in the image below.
When a perforating vein is the primary site of reflux, dilatation of the vessel proceeds both proximally and distally. When dilatation reaches the most proximal portion of the vein, the SFJ or the SPJ is often recruited as a secondary point of reflux. Although most large varices are tributaries off of an incompetent GSV or SSV, failed perforating veins or connecting veins can also give rise to independent varices in the great saphenous distribution without involving the saphenous system itself. Identifying the originating point and the primary pathway of reflux in the thigh is often difficult, which is why duplex ultrasonography has become so helpful in varicose vein workup.
Incompetence of the perforating veins leads to hydrodynamic pressure. The calf pump mechanism helps to empty the deep venous system, but if perforating vein valves fail, then the pressure generated in the deep venous system by the calf pump mechanism are transmitted into the superficial system via the incompetent perforating veins.
Once venous hypertension is present, the venous dysfunction continues to worsen through a vicious circle. Pooled blood and venous hypertension leads to venous dilatation, which then causes greater valvular insufficiency. Over time, with more local dilatation, other adjacent valves sequentially fail, and after a series of valves has failed, the entire superficial venous system is incompetent. As mentioned before, this can then cause subsequent perforator and deep venous valvular dysfunction. The inciting etiology of superficial valvular insufficiency is often difficult to determine because the clinical manifestations of venous hypertension are delayed The clinical findings of varicose veins, reticular veins, and telangiectasias are due to the hypertension in the superficial venous system that spreads to collateral veins and tributary veins, causing dilated tortuous structures. Treatment modalities are geared towards correcting the superficial venous hypertension
At times, the degree or venous hypertension does not correlate to the clinical findings. The presence and size of visible varicosities are not reliable indicators of the volume or pressure of venous reflux. A vein that is confined within fascial planes or is buried beneath subcutaneous tissue can carry massive amounts of high-pressure reflux without being visible at all. Conversely, even a small increase in pressure can eventually produce massive dilatation of an otherwise normal superficial vein that carries very little flow.
In contrast to the superficial veins, the deep veins do not become excessively distended. They can withstand the increased pressure because of their construction and the confining fascia.
Source emedicine.com
Duc Tin Surgical Clinic
Tin tức liên quan

Performance diagnostique de l’interféron gamma dans l’identification de l’origine tuberculeuse des pleurésies exsudatives

A Mixed Phenotype of Airway Wall Thickening and Emphysema Is Associated with Dyspnea and Hospitalization for Chronic Obstructive Pulmonary Disease.

Radiological Approach to Asthma and COPD-The Role of Computed Tomography.

Significant annual cost savings found with UrgoStart in UK and Germany

Thrombolex announces 510(k) clearance of Bashir catheter systems for thromboembolic disorders
Phone: (028) 3981 2678
Mobile: 0903 839 878 - 0909 384 389