







Background
A renal artery aneurysm (RAA) is defined as a dilated segment of renal artery that exceeds twice the diameter of a normal renal artery. Symptomatic RAAs can cause hypertension, pain, hematuria, and renal infarction.
Asymptomatic RAAs may seem benign, but the potential for rupture and fistulization increases with size. Asymptomatic patients can be referred for elective repair, but if patients are symptomatic, further investigation with possible surgical intervention should be considered.
The first published report of an RAA was in 1770 by Rouppe, who described the demise of a sailor who fell onto his right flank. Autopsy revealed a large false aneurysm with rupture. Since that time, many more case reports and case series have provided most of the data on this rare pathologic entity.
Anatomy
The renal arteries arise from the aorta at the level of the intervertebral disc between L1 and L2. Cadaveric studies have shown that more than one renal artery is present in 15% and 20% of cases on the right and left sides, respectively.
A great deal of variety can be found in the anatomy of the renal artery and its branches, but most often the main renal artery splits into an anterior and a posterior division. Within the hilum, the anterior division gives rise to apical, anterior, and inferior segmental branches. Segmental vessels then penetrate the renal parenchyma to become lobar, interlobar, arcuate, or interlobular arteries or afferent arterioles, then finally reach the capillaries and glomeruli.
Measurements of renal artery diameter can differ, depending on the imaging modality used. In one study, ultrasonography reported mean renal artery measurements of 5.04 ± 0.74 mm; with angiography, they were found to be 5.68 ± 1.19 mm. In this study, the authors also determined that when accessory renal arteries were identified, the main renal artery measurements were significantly smaller in diameter than when one renal artery was present.
RAAs can be classified in relation to the parenchyma of the kidney (see the image below). Extraparenchymal aneurysms predominate, comprising approximately 85% of all RAAs. The other 15% are intraparenchymal. Of the extraparenchymal type, roughly 70% are saccular, 20% are fusiform, and 10% are dissecting.
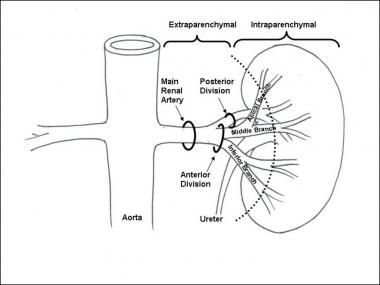
Schematic of renal artery anatomy. The aneurysm location can be classified as extraparenchymal or intraparenchymal.
Of patients with RAAs, 20% present with bilateral pathology, and 30% have multiple aneurysms. RAAs occur with equal frequency in men and women, though ruptures are more common in reproductive-aged women.
Pathophysiology
In true aneurysms, a weakening then dilatation of all layers of the arterial wall occurs. In fibromuscular dysplasia (FMD), the degenerative fibroplasia-type changes lead to this wall weakening. Often, renal artery stenosis is associated. Most patients with FMD are healthy, young, hypertensive women, and on angiography the renal artery appears as a string of beads, with the aneurysm at the renal artery bifurcation.
Ehlers-Danlos syndrome is an autosomal dominant disorder characterized by fragility of medium-sized and large arteries due to type III procollagen deficiency. This condition leads to dissections and aneurysms in any artery, including the renal arteries.
In false aneurysms, or pseudoaneurysms, there is a focal disruption in one or every layer of the artery that causes a saccular outpouching at the weaken area. In blunttrauma, anterior displacement of the relatively mobile kidneys with rapid deceleration generated tension generated in the vascular pedicle causing a fracture of the intima, predisposing it to subintimal dissection then aneurysmal degeneration. Another mechanism involves direct arterial wall contusion against the vertebral bodies.
Anastomotic leaks from previous renal artery reconstructive procedures become walled off by the body, creating a pseudoaneurysm. In this situation, the wall of the aneurysm contains only fibrotic/inflammatory tissue. Iatrogenic endovascular-related aneurysms are caused by intimal trauma and focal dissection, leading to aneurysmal degeneration. Spontaneous renal artery dissections cause aneurysms by the same mechanism described above.
Intraparenchymal aneurysms are believed to arise primarily from inflammatory changes of the vessel wall. These commonly develop into microaneurysms. Intrarenal aneurysms are usually found in multiples and are often associated with arteriovenous fistulas.
Although pregnancy is not associated with an increased incidence of RAA formation, it is associated with a higher rate of rupture. The increased blood flow, intra-abdominal pressure, and vessel wall changes due to the hormonal and metabolic changes associated with gestation are believed to be contributory. Most ruptures occur late in the pregnancy (usually in the third trimester) and are left renal artery–predominant.
In the pediatric age group, RAAs are due to trauma, infection, arteritides, Kawasaki disease, or vascular dysplasias. Multiple idiopathic arterial aneurysms that include renal artery involvement have been described but are extremely rare.
Source emedicine.com
Duc Tin Surgical Clinic
Tin tức liên quan

Performance diagnostique de l’interféron gamma dans l’identification de l’origine tuberculeuse des pleurésies exsudatives

A Mixed Phenotype of Airway Wall Thickening and Emphysema Is Associated with Dyspnea and Hospitalization for Chronic Obstructive Pulmonary Disease.

Radiological Approach to Asthma and COPD-The Role of Computed Tomography.

Significant annual cost savings found with UrgoStart in UK and Germany

Thrombolex announces 510(k) clearance of Bashir catheter systems for thromboembolic disorders
Phone: (028) 3981 2678
Mobile: 0903 839 878 - 0909 384 389